Bibliography for
Exercise Science ISU
Atlantoaxial Instability in Down
Syndrome . (n.d.). Atlantoaxial Instability in Down Syndrome.
Retrieved June 10, 2014, from
http://emedicine.medscape.com/article/1180354-overview
Autism Behavior Problems. (n.d.). : What's
Triggering Your Child's Outbursts?. Retrieved June 9, 2014, from
http://www.helpguide.org/harvard/autism_revolution.htm
Bowerman, B. (n.d.). 13 Motivational Sports
Quotes from Olympic Coaches | Reader's Digest. Reader's Digest.
Retrieved June 10, 2014, from
http://www.rd.com/slideshows/13-motivational-sports-quotes-from-olympic-coaches/#ixzz34ILlTDQk
Bowman-Kruhm, M. (2000). Everything you need
to know about Down syndrome. New
York
Tomorrow. (n.d.). Receiving a Down Syndrome
Diagnosis. Learning Index Page |: Brighter Tomorrows Down Syndrome Education
:|. Retrieved May 22, 2014, from
http://www.brightertomorrows.org/learning.html?language=1
Down Syndrome Society. (n.d.). Your Child with
Down Syndrome. Canadian Down Syndrome Society. Retrieved May 22, 2014,
from
http://www.cdss.ca/images/pdf/brochures/english/your_child_with_down_syndrome_english.pdf
Child with Autism. (n.d.). Child with Autism.
Retrieved June 11, 2014, from http://childwithautism.wordpress.com/
Children, Epilepsy, and Playing Sports: Limits,
Safety, and More. (n.d.). WebMD. Retrieved June 9, 2014, from
http://www.webmd.com/epilepsy/guide/children-sports-safety
Colin Farrell: Special Olympics World Games
2003 “extraordinary experienceâ€. (2013, June 16). The Score.
Retrieved June 9, 2014, from
http://www.thescore.ie/10-year-anniversary-special-olympics-ireland-colin-farrell-video-951469-Jun2013/
Consensus of the Fragile X Clinical &
Research Consortium on Clinical Practices. (n.d.). Fragile X Clinical
Research Consortium. Retrieved June 9, 2014, from
http://www.fragilex.org/wp-content/uploads/2012/08/Physical-Problems-in-FXS2012-Oct.pdf
David Egan:Finding His Voice. (n.d.). Olympics.
Retrieved June 9, 2014, from
http://www.specialolympics.org/Regions/north-america/News-and-Stories/Stories/David-Egan--Finding-His-Voice.aspx
Diagnosis and Management of Fragile X Syndrome.
(n.d.). Diagnosis and Managment of Fragile X Syndrome. Retrieved June 9,
2014, from http://www.aafp.org/afp/2005/0701/p111.html
Down Syndrome news. (n.d.). NDSC Centre.
Retrieved May 24, 2014, from http://www.ndsccenter.org/worpsite/wp-content/uploads/2014/03/DSN-V37N1-WEB.pdf
Down syndrome. (n.d.). Symptoms.
Retrieved June 8, 2014, from
http://www.mayoclinic.org/diseases-conditions/down-syndrome/basics/symptoms/con-20020948
Dr. Anthony Alessi: Sports can help Autistic
Children. (n.d.). Dr. Anthony Alessi: Sports can help Autistic Children.
Retrieved June 10, 2014, from http://www.autismfamilyonline.com/public/613.cfm
Epilepsy and exercise - Better Health Channel.
(n.d.). Better Health Channel. Retrieved June 9, 2014, from http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Epilepsy_and_exercise
Facts about Down Syndrome. (2013, November 6). Centers
for Disease Control and Prevention. Retrieved June 8, 2014, from
http://www.cdc.gov/ncbddd/birthdefects/downsyndrome.html
Farther Off the Wall. (n.d.). Farther Off
the Wall. Retrieved June 11, 2014, from
http://www.insidesocal.com/tomhoffarth/2011/09/14/the-stars-align/
Febrile Seizures Guide: Causes, Symptoms and
Treatment Options. (n.d.). Febrile Seizures Guide: Causes, Symptoms and
Treatment Options. Retrieved June 11, 2014, from
http://www.drugs.com/health-guide/febrile-seizures.html
Fragile X Syndrome (Fragile X-associated
Disorders). (n.d.). National Fragile X Foundation RSS. Retrieved June
10, 2014, from http://www.fragilex.org/fragile-x-associated-disorders/fragile-x-syndrome/
Fragile X Syndrome . (n.d.). Fragile X
Syndrome. Retrieved June 9, 2014, from
http://emedicine.medscape.com/article/943776-overview
Fragile X syndrome. (n.d.). Genetics Home
Reference. Retrieved June 10, 2014, from
http://ghr.nlm.nih.gov/condition/fragile-x-syndrome
Down Syndrome Foundation. (n.d.). FAQ and Facts
about Down Syndrome - Global Down Syndrome Foundation. Global Down Syndrome
Foundation. Retrieved May 20, 2014, from
http://www.globaldownsyndrome.org/about-down-syndrome/facts-about-down-syndrome/
Hayden Schunk saying the Special Olympic Oath.
(n.d.). YouTube. Retrieved June 11, 2014, from
https://www.youtube.com/watch?v=nD5j1vtSTMs
Health Supervision for Children With Fragile X
Syndrome. (n.d.). Health Supervision for Children With Fragile X Syndrome.
Retrieved June 9, 2014, from
http://pediatrics.aappublications.org/content/127/5/994.long
How It All Began. (n.d.). Special Olympics: History
of Special Olympics. Retrieved June 8, 2014, from
http://www.specialolympics.org/history.aspx
Joosa, E., & Bertheleson, D. (n.d.).
Parenting a Child With Down Syndrome: A
Phenomenographic Study. OADD. Retrieved May 22, 2014, from
http://www.oadd.org/publications/journal/issues/vol12no1supp2/download/joosa_berthelsen.pdf
Kohen, D., Uppal, S., Guevremont, A., &
Cartwright, F. (n.d.). Children with disabilities and the educational system
— a provincial perspective. Children with disabilities and the educational
system — a provincial perspective. Retrieved May 22, 2014, from
http://www.statcan.gc.ca/pub/81-004-x/2007001/9631-eng.htm
McNally, D. (n.d.). Quotes on COMMITMENT. Commitment
Quotes. Retrieved June 10, 2014, from http://www.leadershipnow.com/commitmentquotes.html
MedCare Cares!. (n.d.). : Atlanto-Axial
Instability and Children with Down Syndrome. Retrieved June 11, 2014, from
http://medcarepediatrics.blogspot.ca/2013/04/atlanto-axial-instability-and-children.html
Melillo, R. (2013). Autism: the scientific
truth about preventing, diagnosing, and treating autism spectrum disorders-and
what parents can do now. New York
Michael Cox. (n.d.). Courier Mail.
Retrieved June 9, 2014, from http://www.couriermail.com.au/questnews/south/swimmer-michael-cox-will-not-let-down-syndrome-stand-in-his-way-as-he-seeks-more-success-in-the-pool/story-fn8odwua-1226444188224
Down Syndrome Society. (n.d.). Caring for Your
Family. - National Down Syndrome Society. Retrieved May 22, 2014, from
http://www.ndss.org/Resources/Caring-for-Your-Family/
Oaths and Codes of Conduct - Special Olympics North Carolina North Carolina
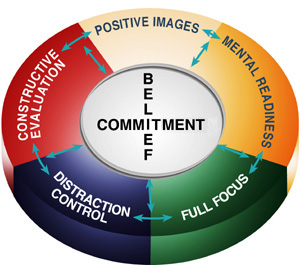
Orlick, T. (n.d.). The Wheel of Excellence. Zone
of Excellence -. Retrieved June 10, 2014, from
http://www.zoneofexcellence.ca/free/wheel.html
Out of the Shadows: Events Leading to the
Founding of The Special Olympics. (n.d.). Special Olympics. Retrieved
June 10, 2014, from http://www.specialolympics.org/Sections/What_We_Do/Out_of_the_Shadows__Events_Leading_to_the_Founding_of_Special_Olympics.aspx
Position Statement on Atlanto-axial Instability.
(n.d.). NDSC Centre. Retrieved June 8, 2014, from
http://ndsccenter.org/worpsite/wp-content/uploads/2012/02/AtlantoAxial_Instability.pdf
Participation by individuals with Down Syndrome
who have Atlantoaxial Instability. (n.d.). Special Olympics. Retrieved
June 9, 2014, from
http://www.specialolympics.ab.ca/uploads/files/Documents/Policy/M-3001%20Atlantoaxial%20Instability.pdf
Physical Problems in Fragile X Syndrome .
(n.d.). Fragile X. Retrieved June 9, 2014, from
http://www.fragilex.org/wp-content/uploads/2012/08/Physical-Problems-in-FXS2012-Oct.pdf
Physical features of autism spectrum disorder
(ASD). (n.d.). KevinMD.com. Retrieved June 10, 2014, from
http://www.kevinmd.com/blog/2010/07/physical-features-autism-spectrum-disorder-asd.html
Pueschel, S. M. (1990). A parent's guide to
Down syndrome: toward a brighter future. Baltimore
Royston, A. (2010). Explaining Down syndrome.
Mankato , Minn.
Santomauro, J. (2011). Friendships. Autism
All-Stars (pp. 83-85). London and Philadelphia
Small Steps, Great Strides - Eunice Kennedy
Shriver. (n.d.). Small Steps, Great Strides - Eunice Kennedy Shriver.
Retrieved June 9, 2014, from http://www.eunicekennedyshriver.org/bios/si
Special Olympics Gymnastics 2012 USA
Championship Gala (Gabriel Beauchamp).mp4. (n.d.). YouTube. Retrieved
June 11, 2014, from https://www.youtube.com/watch?v=u6-w7hmUDvQ
Special Olympics: Frequently-Asked-Questions.
(n.d.). Special Olympics: Frequently-Asked-Questions. Retrieved June 9,
2014, from
http://www.specialolympics.org/Common/Frequently-Asked-Questions.aspx#.U5Xp-nJdXII
Special Olympics: Special Olympics Program
Locator. (n.d.). Special Olympics: Special Olympics Program Locator.
Retrieved June 10, 2014, from
http://www.specialolympics.org/program_locator.aspx
Special Olympics: Sports and Games. (n.d.). Special
Olympics: Sports and Games. Retrieved June 9, 2014, from
http://www.specialolympics.org/sports.aspx
Sports & Exercise | Down Syndrome WA Down
Syndrome WA
Statistics about Down Syndrome. (n.d.). -
RightDiagnosis.com. Retrieved May 20, 2014, from
http://www.rightdiagnosis.com/d/down_syndrome/stats.htm
The Beauty of Chaos. (n.d.). : Lesson 3:
Down Syndrome testing. Retrieved June 11, 2014, from
http://asal-sakti.blogspot.ca/2008/12/down-syndrome-testing.html
Timeline Photos - Special Olympics | Facebook.
(n.d.). Timeline Photos - Special Olympics | Facebook. Retrieved June
11, 2014, from https://www.facebook.com/photo.php?fbid=10152951432728782&set=pb.10331123781.-2207520000.1402462225.&type=3&theater
Tocci, S. (2000). The Family, The Future, Myths
and Truths. Down syndrome (pp. 94-130). New York
Training and Certification. (n.d.). Special
Olympics Canada
Weber, J. D. (2000). Children with fragile X
syndrome: a parents' guide. Bethesda ,
MD
What Is Fragile X Syndrome?. (n.d.). Special
Olympics: FragileX. Retrieved June 9, 2014, from
http://www.specialolympics.org/Sections/Who_We_Are/FragileX.aspx
What is Down syndrome?. (n.d.). Alzheimer
Society of Toronto
What is the Healthy Athletes Program. (n.d.). healthy
athletes program. Retrieved June 11, 2014, from
http://www.sotx.org/programs/healthy-athletes-program.html
Who Are Our Athletes?. (n.d.). Special
Olympics: Our Athletes. Retrieved June 9, 2014, from
http://www.specialolympics.org/athletes.aspx
A division of Future Horizons, Inc.. (n.d.). Autism
Aspergers Digest RSS. Retrieved June 10, 2014, from
http://autismdigest.com/sports-and-autism-thinking-outside-the-bounds/